

Abstract
Introduction: Allogeneic hematopoietic stem cell transplantation (HCT) is the only curative therapy for myelofibrosis (MF). Consideration of HCT is recommended by international working groups and national guidelines for MF patients (pts) age <70 with intermediate-1 with adverse indicators, intermediate-2 or high-risk disease by the Dynamic International Prognostic Scoring System (DIPSS) for MF- a recommendation made in the absence of clear data indicating the optimal timing of HCT for MF. In this large multicenter retrospective study, we analyze overall survival in MF pts treated with and without HCT.
Methods: Disease characteristics, treatments, and outcome data from MF pts receiving non-transplant therapy at 14 US academic medical centers between 2000-2014 were retrospectively collected. MF pts who underwent HCT were identified from the Center for International Blood and Marrow Transplant Research (CIBMTR). The Cox proportional hazards model was used. The reference time point (time zero) was time of referral for the non-transplant (non-HCT) arm and the time of transplant for the HCT arm. The main effect variable (HCT vs. non-HCT) violated the proportionality assumption where comparing to non-HCT, mortality was higher with HCT in early time period from time zero but then was lower in late time period; therefore, the comparison is presented as early time period and late time period. The Cox model identified 14 months from time zero as the ideal cut point to define early and late time periods. The proportionality assumption is satisfied within each of these two periods.
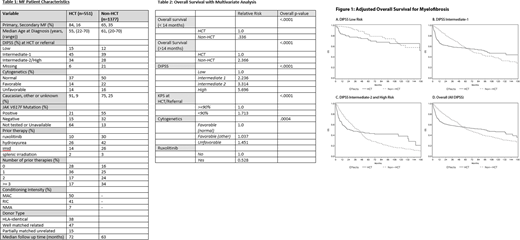
Results: A total of 1377 and 551 pts were included in the non-HCT and HCT arms, respectively (Table 1). In the overall cohort, survival was higher with non-HCT vs. HCT in early time period (relative risk [RR]: 0.34, P< .0001, Figure 1D), but in late time period survival was lower with non-HCT vs. HCT (RR: 2.37, P< 0.001) (Table 2). In the DIPSS low-risk MF group, while survival was higher with non-HCT vs. HCT in the early time period (RR: 0.19, P=0.007, Figure 1A), survival was lower with non-HCT in the late time period, but the latter did not reach statistical significance (RR: 1.45, P=0.39). In the DIPSS intermediate-1 risk group, a survival advantage was present with non-HCT treatments vs. HCT in the early time period (RR: 0.27, P < .0001, Figure 1B), however survival was lower with non-HCT in the late time period (RR: 3.13, P < .0001). Similarly, in those with DIPSS intermediate-2 and high-risk MF, survival advantage was observed with non-HCT in the early time period (RR: 0.41, P< .0001, Figure IC), but survival was lower with non-HCT in the late time period (RR: 2.82, P < .0001).
Conclusion: A long-term survival advantage with transplant was observed for pts with intermediate-1 or higher risk MF, but at the cost of potential early mortality. The magnitude of benefit increased as DIPSS risk score increased. Although this retrospective study has limitations, the results have an impact on clinical practice by suggesting that transplantation could be considered earlier in the disease course and supports the recommendation for consideration of HCT in the setting of intermediate-1 risk MF.
Gowin:Incyte: Consultancy, Other: Scientific Advisory Board, Speakers Bureau. Verstovsek:Celgene: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Incyte: Consultancy; Italfarmaco: Membership on an entity's Board of Directors or advisory committees. Ali:Incyte Corporation: Membership on an entity's Board of Directors or advisory committees. Gupta:Novartis: Consultancy, Honoraria, Research Funding; Incyte: Research Funding. Gerds:Celgene: Consultancy; Apexx Oncology: Consultancy; CTI Biopharma: Consultancy; Incyte: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal